![]()
Since epidemiological week 26, ending 2 July 2023, Nigeria has recorded an unusual increase in cases of diphtheria across several states. From 30 June to 31 August 2023, a total of 5898 suspected cases were reported from 59 Local Government Areas (LGAs) in 11 states. In week 34 (ending 27 August 2023), 234 suspected cases have been reported from 20 LGAs in five states, with one Lab confirmed case1 from the 22 samples collected. Eighteen of these cases were epidemiologically linked 2 and 141 were classified as clinically compatible.
Diphtheria is a highly contagious vaccine-preventable disease caused mainly by the bacteria Corynebacterium diphtheriae which can be fatal in 5-10% of cases, with a higher mortality rate in young children.
WHOs most recent risk assessment of the diphtheria outbreak in Nigeria has maintained the risk as high at the national level, and low at the regional and global levels. Public health measures such as vaccination response, enhanced surveillance for early case detection, case management and risk communication coordinated by the Nigeria Centre for Disease Control (NCDC), in collaboration with WHO and other partners, are being implemented in response to the outbreak.
Description of the situation
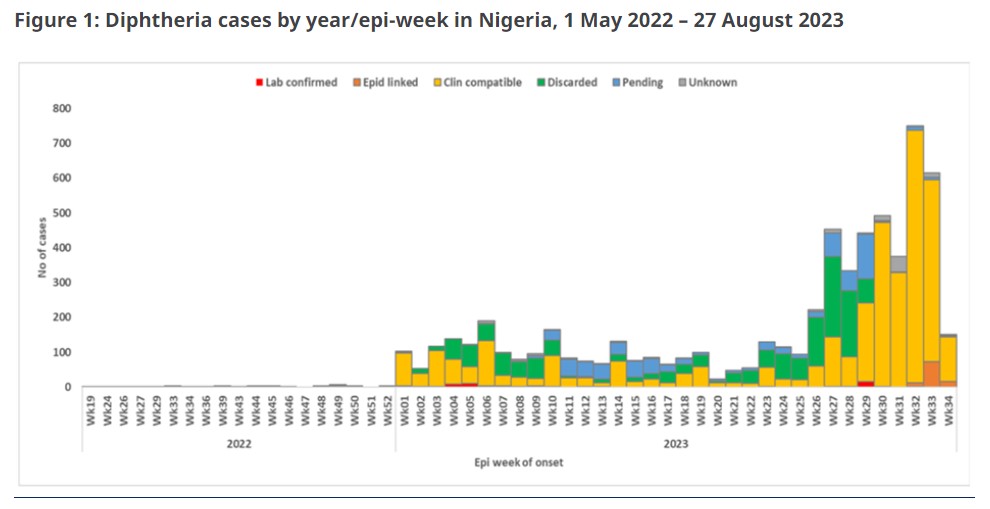
Since the last Disease Outbreak News on diphtheria in Nigeria was published on 27 April 2023, the country has reported suspected cases of diphtheria weekly to WHO. However, between 30 June and 31 August 2023, Nigeria recorded an unusual increase in the number of confirmed diphtheria cases4 (figure 1). From 30 June to 31 August 2023, a total of 5898 suspected cases were reported from 59 LGAs in 11 states across the country. The majority (99.4%) of suspected cases were reported from Kano (1816), Katsina (234), Yobe (158), Bauchi (79), Kaduna (45) and Borno (33).
Of the cumulative 8353 suspected cases reported since the outbreak was first reported in 2022, 4717 (56.5%) cases were confirmed4 (lab confirmed1 (169; 3.6%), epidemiologically linked2 (117; 2.5%) and clinical compatibility3 (4431; 93.9%)). While 1857 (22.2%) were discarded as not compatible with diphtheria, 1048 (12.5%) cases are pending classification and 731 (8.8%) cases had unknown diagnosis. The case fatality ratio dropped slightly from 6.7% during the last update to 6.1%. Of the 4717 confirmed cases, 3466 (73.5%) were aged 1 – 14 years, of these 699 were aged 0-4 years, 1505 aged 5-9 years, 1262 (aged 10 – 14 years. More than half of the cases (2656; 56.3%) were females. Only 1074 (22.8%) of the confirmed cases were fully vaccinated against diphtheria, 299 (6.3%) were partially vaccinated. More than half of the cases (2801; 59.4%) were unvaccinated.
Definitive diagnosis through laboratory molecular testing identified Corynebacterium diphtheriae and Corynebacterium ulcerans isolates as the species driving this outbreak, particularly C. diphtheria as the major etiologic pathogen associated with the current outbreak. Antibiotic susceptibility tests for 62 isolates of C. diphtheriae have been carried out and the findings revealed that all isolates were resistant to penicillin, and most were resistant to trimethoprim-sulfathiazole and ciprofloxacin, while being susceptible to erythromycin. Thus, erythromycin became the drug of choice in the management of this outbreak (Figure 2).

Epidemiology of diphtheria
Diphtheria is a highly contagious vaccine-preventable disease caused mainly by Corynebacterium diphtheria but also by Corynebacterium ulcerans. It spreads between people mainly by direct contact or through the air via respiratory droplets. The disease can affect all age groups; however, unimmunized children are most at risk.
Symptoms often come on gradually, beginning with a sore throat and fever. In severe cases, the bacteria produce a poison (toxin) that causes a thick grey or white patch at the back of throat. This can block the airways, making it hard to breathe or swallow, and also creates a barking cough. The neck may swell in part due to enlarged lymph nodes.
Treatment involves administering diphtheria antitoxin (DAT) as well as antibiotics. Vaccination against diphtheria has been effective in reducing the mortality and morbidity from diphtheria dramatically. Diphtheria is fatal in 5-10% of cases, with a higher mortality rate in young children. However, in settings with poor access to diphtheria antitoxin, the CFR can be as high as 40%.
Nigeria has recorded diphtheria outbreaks in the past, notably in 2011 and 2022. In 2023, a previous outbreak of diphtheria was recorded between January and April 2023 affecting 21 of the 36 states and the FCT. Details of the outbreak have been published on Disease Outbreak News.
Public health response
Coordination: WHO Country Office Incident Management System revised, National Emergency Operation Centre (EOC) activated likewise state EOC in the diphtheria high burden Kaduna, Katsina, Borno; partners mapping ongoing.
Surveillance: Terms of reference for the pillar developed, regular follow up with the states to submit weekly situation report and line-list; WHO and other partners supported NCDC to develop contact tracking and harmonized line-list forms; database for states reporting on response activities p; dashboard for monitoring and evaluation of the response in development;
Laboratory: procurement of commodities; activation of Kano lab to perform testing and culture at state level, transportation of samples;
Vaccination: reactive vaccination Kano (phase 1 & 2), Katsina, Bauchi, Yobe, Kaduna (phase 1);
Risk Communication and Community Engagement: engagement with community leaders, community awareness, development Information Education and Communication material, monitoring rumors, airing jingles, etc.
Case management: supported development of national guideline for case management and surveillance; provided technical guidance on case management; deployed ear, nose and throat (ENT) specialists to treatment centers;
Infection Prevention Control: monitoring of treatment centers on IPC measures is being undertaken;
Operation Support and Logistics: procurement of 10 050 vials diphtheria antitoxin, 15 000 vial erythromycin ETA 28/08 and lab commodities; prepared delivery plan of Personal Protection Equipment to priority states;
Preventing and Responding to Sexual Exploitation, Abuse and Harassment: conducted PRSEAH risk assessment.
Staff health security and wellbeing: general security briefings, reporting template, FAQ on diphtheria
WHO risk assessment
Diphtheria is a vaccine-preventable disease caused mainly by exotoxin-producing Corynebacterium diphtheriae but also by Corynebacterium ulcerans. Diphtheria is fatal in 5 - 10% of cases, with a higher mortality rate in young children. Treatment involves administering DAT as well as antibiotics. Vaccination against diphtheria reduces the mortality and morbidity of diphtheria dramatically.
Nigeria is currently facing a second wave of a diphtheria outbreak after a first wave of the outbreak was recorded between epidemiological week 52, 2022 (1 January 2023) and week 20, 2023 (22 May 2023). There is an increase in the affected population with a rise in the number of confirmed cases and related deaths reported in epidemiological weeks 31-33. There is an increased risk of transmission, with clusters and outbreaks reported in newly affected LGAs, with currently 27 LGAs reporting one clinically compatible case in the last three reporting weeks relative to 15 LGAs that had active case in the preceding three weeks.
The low national coverage (57%) of the Pentavalent vaccine (Penta 3) administered in routine immunization, and the suboptimal vaccination coverage in the pediatric population—with 43% of the target population unvaccinated—underscores the risk of further spread and the accumulation of a critical mass of susceptible population in the country with sub-optimal herd or population immunity. Vaccine coverage of 80–85% must be maintained to ensure community protection.
This emphasizes the urgent need to strengthen diphtheria vaccination coverage nationwide, especially in the most affected states, such as Kano. Additionally, particular attention is necessary for regions experiencing insecurity challenges, like the Northwest, as it hampers vaccine accessibility. Due to insecurity, especially in Northeast Nigeria, vaccination coverage remains suboptimal.
DAT supply is currently very constrained and insufficient to respond to current demands, as there is only a limited number of manufacturers and large outbreaks are being reported in different regions of the world. The NCDC, with support from WHO and other partners have procured 10 050 DAT vials for case management in response to the outbreak.
Diphtheria outbreaks are underreported in Nigeria. According to the 2021 Nigeria Multiple Indicator Cluster Survey and National Immunization Coverage Survey, the third dose of pentavalent vaccine (Penta3) coverage was 57% in 2021.
WHO second Rapid Risk Assessment for diphtheria in Nigeria reassessed and maintained the risk as high at the national level and low at the regional and global levels.
WHO advice
The control of diphtheria is based on primary prevention of disease by ensuring high population immunity through vaccination, and secondary prevention of spread by the rapid investigation of close contacts to ensure prompt treatment of those infected.
Epidemiological surveillance ensuring early detection of diphtheria outbreaks should be in place in all countries, and all countries should have access to laboratory facilities for reliable identification of toxigenic C. diphtheriae. Adequate quantities of diphtheria antitoxin should be available nationally or regionally for the medical management of cases.
Vaccination is key to preventing cases and outbreaks, and adequate clinical management involves administering diphtheria anti-toxin to neutralize the toxin and antibiotics reducing complications and mortality.
WHO recommends early reporting and case management of suspected diphtheria cases to initiate the timely treatment of cases, and follow-up of contacts, and ensuring a supply of diphtheria antitoxin.
WHO advises implementing the following Infection Prevention & Control measures in health care settings:
1) Apply standard precautions, with focus on hand hygiene, personal protective equipment and equipment and environmental cleaning and disinfection droplet and contact precautions (at all times).
2) At screening/triage, immediately place patients with symptoms of Upper Respiratory Tract Infection in a separate area until examined, and, if a suspected case, cohorted with patients with the same diagnosis. Keep the isolation area segregated from other patient-care areas.
3) Maintain one meter between patients. Keep patient care areas well ventilated.
4) Avoid patient movement or transport out of isolation area. If movement is necessary out of isolation area, have patient use a medical mask and cover any wounds/lesions on patient’s body.
The case management should be carried out following the WHO guidelines. In addition, high-risk populations such as young children under five years of age, school children, the elderly, close contact with diphtheria cases, and healthcare workers should be vaccinated on a priority basis. A coordinated response and community engagement can support further transmission and control of the ongoing outbreak.
Prophylactic antibiotics (penicillin or erythromycin, dependent on drug sensitivity) are indicated for close contacts of confirmed cases for seven days. If the culture is positive for toxigenic Corynebacterium spp., then the contact should be treated as a case with an antibiotic course for two weeks (DAT is not needed for asymptomatic cases or cases without a pseudomembrane).
Although travelers do not have a special risk of diphtheria infection, it is recommended that national authorities remind travelers going to areas with diphtheria outbreaks to be appropriately vaccinated in accordance with the national vaccination scheme established in each country prior to travel. A booster dose is recommended if more than five years have passed since their last dose.
About WHO
The World Health Organization provides global leadership in public health within the United Nations system. Founded in 1948, WHO works with 194 Member States, across six regions and from more than 150 offices, to promote health, keep the world safe and serve the vulnerable. Our goal for 2019-2023 is to ensure that a billion more people have universal health coverage, to protect a billion more people from health emergencies, and provide a further billion people with better health and wellbeing.