Dr Mansukh Mandaviya, Union Minister for Health and Family Welfare visited Safdarjung Hospital today and had an informal interactive session with Heads of Departments and Staff of Safdarjung Hospital and Vardhman Mahavir Medical College. He spent more than 2.5 hours with the heads of various departments, nurses, heads of security and sanitation services and listened with patience to their numerous suggestions on quality hospital management, clinical practices, infection control measures, sanitation processes and patient-centered high quality healthcare provision. They shared their experience of working for providing round the clock services to the poor, needy and underprivileged during the pandemic.

The Union Minister emphasized on the best output and performance-oriented work culture through efficient coordination, with the goal of providing highest quality healthcare to the patients. He urged everyone to instill a mentality of accepting criticism and work towards institutional building through shared goals, aims and work culture. “Our goal should be on how to provide the best healthcare to every patient who walks in. When we have clarity on this goal and our resultant role, all our actions will also become clear and action oriented”, he stated. Dr Mandaviya gave a very strong message that there will be zero tolerance to poor standard of work at all levels. “No one should feel that absenteeism and poor performance shall go unnoticed”, he emphasized. The Union Health Minister exhorted all HoDs to evaluate performance and attendance of all employees at all levels including the security and contractual staff to ensure that absenteeism and poor-quality work is effectively addressed. He encouraged the teams in each department to not only achieve superior targets but sustain the high-performance standards. “It is easy to achieve very high performance for a short time, but extremely difficult to sustain such exemplary standards of healthcare delivery”, he noted.

Dr Mandaviya motivated all the teams to work towards converting Safdarjung Hospital into a highly reputed hospital of highest quality. “The Ministry is committed to supporting the hospital in all its endeavour”, he stated.

Dr Mandaviya also advised the HoDs to meet their teams every week, undertake physical visit of all departments and evaluate their performance to ensure best output. Noting that we have a huge advantage due the large number of patients that public sector hospitals treat, the Minister exhorted them to make analytical studies and publish them in reputed and popular journals.
Taking confidence from the efficient handling of the COVID19 pandemic in the country, the Union Minister praised the Indian doctors for leaving an imprint globally. He stated that “it is now time to develop our healthcare model and show to the world our strengths in various aspects of healthcare, pharma and R&D”. He congratulated the hospital for receiving the 1st Kayakalp Award of Rs 3 Crore.
Prof. (Dr.) Sunil Kumar, Director General of Health Services, Dr S V Arya, Medical Superintendant, Safdarjung Hospital, Heads of various departments, Heads of Sanitation and Kayakalp cell were present in the meeting.
Medical Council of India (Professional Conduct, Etiquette and Ethics) Regulations, 2002 provides that every physician should as far as possible prescribe drugs with generic names. Further, the erstwhile Medical Council of India (MCI) had issued Circulars in which all the Registered Medical Practitioners were directed to comply with the aforesaid provisions.
The National Medical Commission (NMC) Act, 2019 empowers Ethics and Medical Registration Board (EMRB) of NMC and the appropriate State Medical Councils to take disciplinary action against a doctor for violation of provisions of the aforesaid Regulations.
The Union Minister of State for Health and Family Welfare, Dr. Bharati Pravin Pawar stated this in a written reply in the LokSabha today.
Under the Pradhan Mantri Bhartiya Janaushadhi Pariyojana (PMBJP) being implemented by the Department of Pharmaceuticals, a medicine is priced on the principle of maximum of 50% of average price of the top three brands of the said medicine. Thus, the prices of Jan Aushadhi Medicines are cheaper at least by 50% and in some cases, by 80% to 90% of the market price of the branded medicines.
Pharmaceuticals & Medical Devices Bureau of India (PMBI), the implementing agency of the Scheme has presently its warehouses situated at Gurugram, Chennai and Guwahati. In addition, there are 39 number of distributors spread all across the country. A total of six warehouses are envisaged by March 2025.
As on 31.01.2022, about 8,675 PMBJP Kendras have been opened in all the districts of the country so as to ensure accessibility of quality affordable generic medicines. In order to ensure availability of medicines, an Information Technology (IT) enabled End-to-End supply chain system with Point-of-Sale (POS) application for value added services has been implemented by PMBI to monitor end to end supply chain management system. All warehouses have SAP based inventory management system and the demand forecasting is done through the said system so as to place orders as per the desired inventory levels.
National Pharmaceutical Pricing Authority (NPPA) under the Department of Pharmaceuticals regulates the prices of all drugs – whether branded or generic. While it fixes the ceiling price of scheduled medicines specified in the first schedule of the Drugs (Prices Control) Order, 2013, in case of non-scheduled medicines, the manufactures are free to fix Maximum Retail Price (MRP) of the drug. However, DPCO provides that the same do not increase by more than 10% of their MRP during the preceding twelve months. The details of retail/ceiling prices fixed/revised by NPPA are available on NPPA’s website, viz., www.nppaindia.nic.in.
PMBI spreads awareness about generic medicines through various types of advertisements such as TV, FM Radio, Auto wrapping, Cinema, Bus Brandings, State Transport Bus Stands, Digital Screen Advertisement at Railway Stations, etc. In addition, PMBI also educates the public regularly about usages of Jan Aushadhi generic medicines through various social media platforms like Facebook, Twitter, Instagram, YouTube, etc. The Bureau also organizes seminars and workshops to spread awareness about the scheme. Further, to propagate achievements of the scheme and create awareness about its benefits Jan Aushadhi Diwas is celebrated every year on 7th March.
The information was given by the Union Minister of Chemicals and Fertilizers, Shri Mansukh Mandaviya in a written reply in the Lok Sabha today.
“Public Health and Hospital” is a state subject, the primary responsibility of ensuring availability of healthcare facilities including access to healthcare facilities in tribal dominated areas lies with the respective State Governments including Madhya Pradesh. However, Ministry of Health and Family Welfare, Government of India provides technical and financial support to the States/UTs to strengthen the public healthcare facilities through NHM.
The National Health Mission (NHM) is a Centrally Sponsored Scheme which envisages achievement of universal access to equitable, affordable & quality health care services that are accountable and responsive to people’s needs. NHM encompasses its two Sub-Missions, the National Rural Health Mission (NRHM) and the National Urban Health Mission (NUHM). The main programmatic components include Health System Strengthening in rural and urban areas, Reproductive-Maternal- Neonatal-Child and Adolescent Health (RMNCH+A), and Communicable and Non-Communicable Diseases.
Under the National Health Mission (NHM), financial and technical support is provided to States/UTs to strengthen their health care systems including setting-up/upgrading public health facilities and augmenting health human resource on contractual basis for provision of equitable, affordable healthcare to all its citizens particularly the poor and vulnerable population in the tribal areas based on requirements posed by the States in their Programme Implementation Plans (PIPs) within their resource envelope.
Various relaxations that are supported under NHM for better healthcare for beneficiaries in tribal areas are as follows;
Ayushman Bharat- Health and Wellness Centres (HWCs) are established by transforming the Sub-Health Centres (SHCs) and Primary Health Centres (PHCs), as part of the Ayushman Bharat - the flagship programme of Government of India, to deliver twelve packages of Comprehensive Primary Health Care (CPHC) that includes preventive, promotive, curative, palliative and rehabilitative services which is universal, free and close to the community. In the current financial year, over 90109 HWCs have been operationalized till 06th February, 2022. Of these, 15041 are in 177 tribal districts.
The population norms for setting up Health Facilities in vulnerable areas are relaxed. Against the population norms of 5,000, 30,000 and 1,20,000 for setting up of SHC, PHC and CHC, the norm is 3,000, 20,000 and 80,000 respectively in vulnerable areas such as remote, tribal, desert and hard to reach areas.
Under NHM, States/UTs have been given flexibility to deploy Mobile Medical Units (MMUs) to provide a range of health care services for the population particularly living in remote, in-accessible, un-served and under-served areas, as per the needs identified by the respective States/UTs.
To minimize the Out-of-Pocket Expenditure incurred on health services, National Free Drugs Service Initiative and National Free Diagnostic Service Initiative have been rolled out. The medicines are provided adequately to all health facilities, including the health facilities in vulnerable areas, as per the essential medicines lists for respective levels of facilities. Special focus is given to ensure that there are no interruptions in availability of medicines in health facilities in vulnerable areas.
The ASHA programme guidelines provide for recruitment of ASHA at habitation level, in hilly, tribal and difficult areas. Consequently, ASHAs have been put in place at habitation level (well below the national norm of one ASHA at a population of about 1000).
Government of India is supporting states in implementation of National Ambulances Services under NHM for free transportation of sick patients to the health facilities. States are free to place these ambulances at a lower population norm or as per time to care approach so that these ambulances are easily accessible by all.
Further, all tribal majority districts whose composite health index is below the State average have been identified as High Priority Districts (HPDs) and these districts receive more resources per capita under the NHM as compared to the rest of the districts in the State. These districts receive higher per capita funding, have enhanced monitoring and focussed supportive supervision and are encouraged to adopt innovative approaches to address their peculiar health challenges.
States are encouraged to adopt flexible norms for engaging specialists for public health facilities by various mechanisms like ‘contracting in’ and ‘contracting out’ of specialist services under National Health Mission. NHM provides for following types of incentives and honorarium to staff for ensuring service delivery in rural and remote areas in the country:
Honorarium to Gynecologists/Emergency Obstetric Care (EmoC) trained, Pediatricians & Anesthetist/ Life Saving Anesthesia Skills (LSAS) trained doctors for conducting C Sections.
Hard Area allowances and special packages are provided to attract health HR, especially medical officers and specialists, to remote and difficult areas.
Incentives like special incentives for doctors, incentive for ANM for ensuring timely ANC checkup and recording, incentives for conducting Adolescent Reproductive and Sexual Health (ARSH) activities etc.
States have also been allowed to offer negotiable salaries to attract Specialists including flexibility in strategies such as ''You quote, we pay".
In addition, non-Monetary incentives such as preferential admission in post graduate courses for staff serving in difficult areas and improving accommodation arrangement in rural areas have also been introduced under NHM.
The Union Minister of State for Health and Family Welfare, Dr. Bharati Pravin Pawar stated this in a written reply in the LokSabha today.
The Government of India has conducted stem cell research through various Departments/ Institutions by supporting basic as well as clinical research through national funding agencies like the Indian Council of Medical Research (ICMR), Department of Biotechnology (DBT) and Department of Science and Technology (DST). The work done in this field has resulted in the establishment of state-of-art infrastructure at over 40 premier health research and educational institutes in addition to supporting industry initiatives in India.
ICMR has released the National Guidelines for Stem Cell Research (NGSCR) 2017 which were framed in harmonization of international guidelines. Government has supported the ethical and scientific conduct of stem cell research through guidelines for stem cell research. Government supports using hematopoietic cell transplantation (HCT) for hematological disorders, as standard of care, as per NGSCR-2017.
ICMR has also released Evidence Based Status of Stem Cell Therapy for Human Diseases for creating awareness and understanding regarding experimental use of stem cells under the purview of clinical trial and the document is available at the following link:
The Government has notified the New Drugs and Clinical Trial Rules, 2019 for regulation of clinical trials and New Drugs including cell & stem cell derived product, gene therapeutics product and xenografts for human use, which contains various provisions for improving transparency and accountability for the approval process and to promote research and development of the new drugs.
The total funds released by Indian Council of Medical Research (ICMR) during last three years under Stem cell research in fellowships and Ad-hoc project, are as below:

The Department of Biotechnology (DBT) has supported projects for basic biology of stem cells; early and late translational research; developing gene editing technology for potential therapeutic applications and creation of animal models for various human diseases. The funds released by the DBT during the last three years and the current year in this area is Rs. 7345.58 Lakh.
The Union Minister of State for Health and Family Welfare, Dr. Bharati Pravin Pawar stated this in a written reply in the LokSabha today.
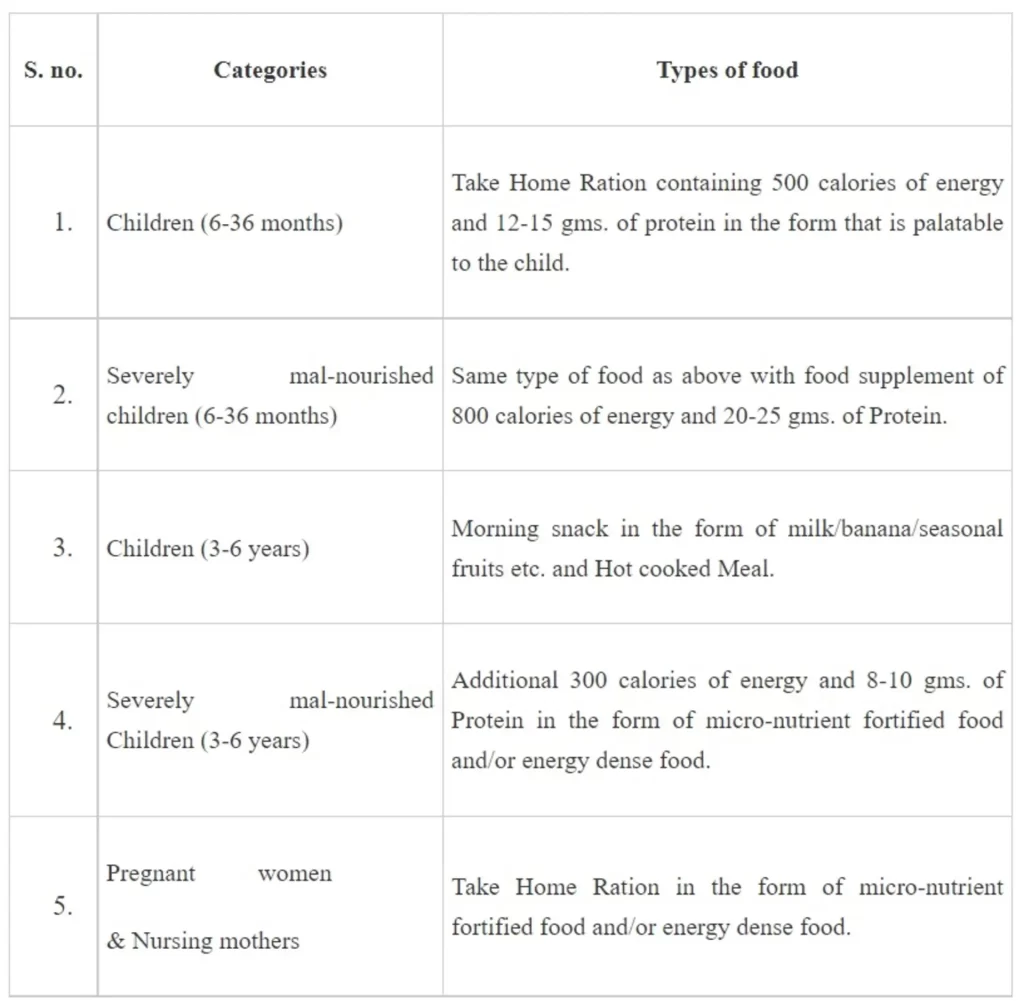
The Government of India is implementing several schemes/programmes of different Ministries/Departments through States/UTs to address various aspects related to nutrition and promoting nutritional diet and a healthy living especially for children across the country. The POSHAN Abhiyaan, Pradhan Mantri Matru Vandana Yojana, Anganwadi Services Scheme and Scheme for Adolescent Girls under the Umbrella Integrated Child Development Services Scheme (ICDS) are implemented by Government as direct targeted interventions to address the problem of malnutrition in the country.
The detail of supplementary nutrition is provided to different categories of the beneficiaries as per the norms for 300 days in a year are through ICDS. The detail are provided below in tabular form.
Under Poshan Abhiyaan ‘Rashtriya POSHAN Maah’ and ‘Poshan Pakhwada’ are celebrated each year in the month of September and March respectively with the aim to create awareness about nutrition and healthy food etc.
Awareness generation activities such as “Eat Right India” campaign are also implemented with the objective to create awareness about ‘Eating Healthy’ ‘Eating Safe’ and ‘Eating Sustainably ‘among school children and the community at large.
Other schemes below implementing for promoting nutritional diet and a healthy living especially for children across the country are:
Pradhan Mantri Poshan Shakti Nirman (PM POSHAN) Scheme earlier known as ‘National Programme for Mid-Day Meal in Schools’ is one of the foremost rights based Centrally Sponsored Schemes. This Scheme covers all school children studying in Classes I-VIII in Government and Government-Aided Schools.
Schedule II of the National Food Security Act (NFSA), mandates provision of hot cooked meal containing 450 calories and 12 gms protein for primary and 700 calories and 20 gms protein for upper primary class children under this scheme. The scheme also provides cooking cost of ₹ 4.97 for primary and ₹ 7.45 for upper primary per child per day on all working days for meeting the cost of pulses, vegetables, edible oil and condiments.
The Union Minister of State for Health and Family Welfare, Dr. Bharati Pravin Pawar stated this in a written reply in the LokSabha today.
Government of India has recognised the potential of Digital Health for strengthening of healthcare delivery system across the country. Toward this, various schemes/programmes have initiated for implementation of digital health initiative.
Ayushman Bharat Digital Mission has been launched to create an enabling environment for implementation of digital health technologies in health domain. Under the ABDM, the three key registries namely Health ID, Health Professional Registry (HPR), Health Facility Registry (HFR) and digital infrastructure for data exchange have been developed. The digital health ecosystem established under ABDM supports seamless exchange of data across primary, secondary, and tertiary facilities to ensure continuum of care. Citizens is benefitted with lower out of pocket expenditure, reduced repeat testing, precision medicine, customized treatment plans, and quality of service across spectrum.
Government of India has also proactively implemented e-Sanjeevani telemedicine platform to provide free of cost teleconsultation services to citizens for COVID as well as Non-COVID ailments. It is operational in 36 States/UTs & provides doctors/specialist medical services to citizens through online consultation mode from the comfort of their homes besides consultations through hub & spoke model in Health & Wellness Centres(HWCs).
The Union Minister of State for Health and Family Welfare, Dr. Bharati Pravin Pawar stated this in a written reply in the RajyaSabha today.
The National Health Authority (NHA) under its flagship scheme of Ayushman Bharat Digital Mission (ABDM) announced completion of 27 major integrations across Government and private sector. These integrations with organizations offering Health Management Information Systems (HMIS), Laboratory Management Information Systems (LMIS), health locker services, health tech services and other digital services are a step towards developing a user-inclusive, integrated and interoperable digital healthcare eco-system for the country.
Launched nationwide on 27th Sept 2021 by the Hon’ble Prime Minister of India, Shri Narendra Modi, ABDM aims to create a seamless online platform that will enable interoperability within the digital healthcare ecosystem. ABDM has developed building blocks and interoperable APIs to offer a seamless digital healthcare experience for all stakeholders – health facilities, patients and healthcare professionals. The digital ecosystem developed is now accessible to health facilities and health tech players for integration.
This integration is a partnership between ABDM and several health tech partners that will help bridge the existing gap amongst different stakeholders of healthcare ecosystem. Currently, the following partners (listed category-wise in the order of their integration completion dates) have received ‘ABDM-integrated’ certificates and logos from NHA for their products integrated with ABDM. These certificates and logos mention the level(s) of integration completed by the product
• HMIS systems like e-Hospital by NIC, e-Sushrut by Centre for Development of Advanced Computing (C-DAC), Medmantra by Apollo Hospitals, MediXcel by Plus91 Technologies Private Limited, EkaCare by Orbi Health, Bahmni by Thoughtworks Technologies, DocOn by DocOn Technologies, Bajaj Finserv Health for Doctors and Bajaj Finserv Health App by Bajaj Finserve Health Limited
• LMIS systems like Centralised Laboratory Information Management Systems (CLIMS) by SRL Limited and CrelioHealth by Crelio Health Software
• Health locker service providers like DigiLocker by National e-Governance Division, DRiefcase by Driefcase Healthtech Pvt Ltd and DocPrime by DocPrime Technologies
• Health Tech players like Practo by Practo Technologies, Verraton Health by Verraton Health Pvt. Ltd, MarSha Health Clinical Decision Support System (CDSS) by MarSha Healthcare, Indian Joint Registry (IJR) by NEC Software Solutions India, PayTM by One97 Communications Limited, JioHealthHub by Reliance Digital Health Limited, Raxa by Raxa Health Information Services Private Limited and Doxper by InformDS Technologies Private Limited
• Other health tech solutions developed by Central and State Governments like CoWIN by Ministry of Health & Family Welfare (MoHFW), Nikshay by Central TB Division, MoHFW, e-Aarogya by Health Department DNH & DD, ANM AP HEALTH app for Andhra Pradesh Medical Staff and EHR by Andhra Pradesh Health and Family Welfare Department, CPHC-NCD Software by National Institute of Health & Family Welfare (NIHFW), Transaction Management System (TMS) and Beneficiary Identification System (BIS) of Pradhan Mantri Jan Arogya Yojana (PM-JAY) by National Health Authority (NHA)
(NOTE: Some products may have features of more than one category of digital health solutions.)
These ABDM integrations of digital platforms in healthcare are achieved through ABDM Sandbox (an experimental digital space which is detached or separated from the actual digital health ecosystem and is created for testing of integration processes before the digital health product is made live for the actual use). Any entity can register on the ABDM Sandbox by following a step-by-step process of integrating and validating their software systems by partnering with the ABDM APIs. So far, about 745 entities have registered on the ABDM Sandbox.
Talking about ABDM’s role, Dr R S Sharma, CEO, NHA said, “The overarching objective of Ayushman Bharat Digital Mission is to deliver health services in an affordable manner with quality and accessibility. These health services should be available everywhere in the country and obviously technology tools will reduce the concept of distance. The system which we are building is an interoperable, open system which is based on open source with open APIs and open standards. So that basically enables every or public player, whosoever wants to integrate with the system to integrate with ABDM.”
Adding further on the progress of integrations done so far, Dr Sharma said, “Out of 27 integrators, 17 integrators are private sector integrators who are actually providing solutions which are compatible with the overall architecture of ABDM. And each application can talk to every other application. So, this is a wonderful architecture which will enable a scalable system.”
The complete list of ABDM partners and their respective integration levels are mentioned at https://abdm.gov.in/home/partners . More information about ABDM Sandbox is available here: https://sandbox.abdm.gov.in/
As per the Global Burden of Disease study, published in Lancet public health, the cases of dementia in India were estimated to be 38,43,118 in the year 2019. The number of cases of dementia in India is not maintained centrally.
Risk for Dementia can be potentially reduced by better management of Diabetes and Hypertension. Government of India is implementing the National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular Diseases and Stroke (NPCDCS) with focus on strengthening infrastructure, human resource development, screening, early detection and management of common Non-Communicable Diseases (NCDs) including diabetes and hypertension. Screening for common NCDs is also an integral part of service delivery under Ayushman Bharat – Health and Wellness Centres. Government is also implementing the National Programme for Health Care of the Elderly (NPHCE). The major activities of NPHCE include setting up of Geriatric Department in regional Geriatric Centres (RGC) with OPD care services and 30 bedded Geriatric Ward, setting up of Geriatric units at District Hospitals to provide specialized Geriatric Services including a 10 bedded Geriatric Ward, establishment of a rehabilitation unit at all Community Health Centres and Geriatric Clinics twice a week, setting up of weekly Geriatric Clinic by trained Medical Officers at Primary Health Centres and information, education and communication activities on healthy lifestyle, home care to the bed ridden and supporting devices for the needy elderly persons at sub-centre level.
Further, to address the burden of mental disorders, the Government is supporting implementation of the District Mental Health Programme (DMHP) under NMHP in 704 districts of the country for detection, management and treatment of mental disorders/ illness. Under the Tertiary care component of National Mental Health Programme, 25 Centres of Excellence and 47 PG Departments have been sanctioned to increase the intake of students in PG departments in mental health specialities as well as to provide tertiary level treatment facilities. The Central and State Mental Health Institutions and the Psychiatric Wings of the Central and State medical colleges also have facilities for early detection and treatment for Alzheimer’s Disease, which is the most common cause of Dementia.
The major steps taken by the Government to curb the use of tobacco in country are as under:
The Ministry of Health & Family Welfare has enacted a comprehensive legislation, namely the Cigarettes and Other Tobacco Products (Prohibition of Advertisement and Regulation of Trade and Commerce, Production, Supply and Distribution) Act, 2003 (COTPA 2003) to discourage the consumption of tobacco products in order to protect the masses from the health hazards attributable to tobacco use. The provisions under COTPA, 2003 and the Rules made thereunder mandates prohibition of smoking in public places; ban on sale of tobacco products to and by minors and within 100 yards of educational institutions; prohibition on direct and indirect advertising of tobacco products and mandatory display of specified health warnings.
The National Tobacco Control Programme (NTCP) was launched by this Ministry in 2007- 08 with the aim to (i) create awareness about the harmful effects of tobacco consumption, (ii) reduce the production and supply of tobacco products, (iii) ensure effective implementation of the provisions under COTPA, 2003 (iv) help people quit tobacco use, and (v) facilitate implementation of strategies for prevention and control of tobacco advocated by WHO Framework Convention of Tobacco Control. Enforcement efforts are also monitored by the State Tobacco Control Cells (STCCs) and District Tobacco Control Cells (DTCCs).
Specified health warnings are displayed on all tobacco products packs covering 85% of the principal display area of tobacco product packs.
Revised guidelines for Tobacco Free Educational Institutions (ToFEI) to implement Section-6 of COTPA, 2003 have been disseminated/implemented.
The Union Minister of State for Health and Family Welfare, Dr. Bharati Pravin Pawar stated this in a written reply in the Rajya Sabha today.
The Fairbank's disease (Multiple epiphyseal dysplasia) patient usually requires management of pain and orthopedic procedures, for which facilities are available at tertiary care institutions in India.
Another rare disorder, Acromegaly is caused by excessive secretion of growth hormone, most often from a tumor in the pituitary gland. The disorder causes increased height when it manifests in childhood and adolescent age group, before the fusion of bony epiphysis.
Both the diseases’ patients are getting treatment at various tertiary health facilities like Medical Colleges, Central Institutes like AIIMS, Central Government hospitals where treatment is available at free or subsidized rates besides in tertiary care private hospitals. The somatostatin drug used for Acromegaly, is a scheduled drug as per the National List of Essential Medicines 2015. Therefore, the National Pharmaceutical Pricing Authority has fixed the ceiling price.
The Union Minister of State for Health and Family Welfare, Dr. Bharati Pravin Pawar stated this in a written reply in the Rajya Sabha today.