The World Health Organization provides global leadership in public health within the United Nations system. Founded in 1948, WHO works with 194 Member States, across six regions and from more than 150 offices, to promote health, keep the world safe and serve the vulnerable. Our goal for 2019-2023 is to ensure that a billion more people have universal health coverage, to protect a billion more people from health emergencies, and provide a further billion people with better health and wellbeing.
New WHO Global Air Quality Guidelines (AQGs) provide clear evidence of the damage air pollution inflicts on human health, at even lower concentrations than previously understood. The guidelines recommend new air quality levels to protect the health of populations, by reducing levels of key air pollutants, some of which also contribute to climate change.
Since WHO’s last 2005 global update, there has been a marked increase of evidence that shows how air pollution affects different aspects of health. For that reason, and after a systematic review of the accumulated evidence, WHO has adjusted almost all the AQGs levels downwards, warning that exceeding the new air quality guideline levels is associated with significant risks to health. At the same time, however, adhering to them could save millions of lives.
Every year, exposure to air pollution is estimated to cause 7 million premature deaths and result in the loss of millions more healthy years of life. In children, this could include reduced lung growth and function, respiratory infections and aggravated asthma. In adults, ischaemic heart disease and stroke are the most common causes of premature death attributable to outdoor air pollution, and evidence is also emerging of other effects such as diabetes and neurodegenerative conditions. This puts the burden of disease attributable to air pollution on a par with other major global health risks such as unhealthy diet and tobacco smoking.
Air pollution is one of the biggest environmental threats to human health, alongside climate change. Improving air quality can enhance climate change mitigation efforts, while reducing emissions will in turn improve air quality. By striving to achieve these guideline levels, countries will be both protecting health as well as mitigating global climate change.
WHO’s new guidelines recommend air quality levels for 6 pollutants, where evidence has advanced the most on health effects from exposure. When action is taken on these so-called classical pollutants – particulate matter (PM), ozone (O₃), nitrogen dioxide (NO₂) sulfur dioxide (SO₂) and carbon monoxide (CO), it also has an impact on other damaging pollutants.
The health risks associated with particulate matter equal or smaller than 10 and 2.5 microns (µm) in diameter (PM₁₀ and PM₂.₅, respectively) are of particular public health relevance. Both PM₂.₅ and PM₁₀ are capable of penetrating deep into the lungs but PM₂.₅ can even enter the bloodstream, primarily resulting in cardiovascular and respiratory impacts, and also affecting other organs. PM is primarily generated by fuel combustion in different sectors, including transport, energy, households, industry, and from agriculture. In 2013, outdoor air pollution and particulate matter were classified as carcinogenic by WHO’s International Agency for Research on Cancer (IARC).
The guidelines also highlight good practices for the management of certain types of particulate matter (for example, black carbon/elemental carbon, ultrafine particles, particles originating from sand and dust storms) for which there is currently insufficient quantitative evidence to set air quality guideline levels. They are applicable to both outdoor and indoor environments globally, and cover all settings.
“Air pollution is a threat to health in all countries, but it hits people in low- and middle-income countries the hardest,” said WHO Director-General, Dr Tedros Adhanom Ghebreyesus. “WHO’s new Air Quality Guidelines are an evidence-based and practical tool for improving the quality of the air on which all life depends. I urge all countries and all those fighting to protect our environment to put them to use to reduce suffering and save lives.”
Disparities in air pollution exposure are increasing worldwide, particularly as low- and middle-income countries are experiencing growing levels of air pollution because of large-scale urbanization and economic development that has largely relied on the burning of fossil fuels.
“Annually, WHO estimates that millions of deaths are caused by the effects of air pollution, mainly from noncommunicable diseases. Clean air should be a fundamental human right and a necessary condition for healthy and productive societies. However, despite some improvements in air quality over the past three decades, millions of people continue to die prematurely, often affecting the most vulnerable and marginalized populations,” said WHO Regional Director for Europe, Dr Hans Henri P. Kluge. “We know the magnitude of the problem and we know how to solve it. These updated guidelines give policy-makers solid evidence and the necessary tool to tackle this long-term health burden.”
Global assessments of ambient air pollution alone suggest hundreds of millions of healthy life years of life lost, with the greatest attributable disease burden seen in low and middle-income countries. The more exposed to air pollution they are, the greater the health impact, particularly on individuals with chronic conditions (such as asthma, chronic obstructive pulmonary disease, and heart disease), as well as older people, children and pregnant women.
In 2019, more than 90% of the global population lived in areas where concentrations exceeded the 2005 WHO air quality guideline for long term exposure to PM₂.₅. Countries with strong policy-driven improvements in air quality have often seen marked reduction in air pollution, whereas declines over the past 30 years were less noticeable in regions with already good air quality.
The goal of the guideline is for all countries to achieve recommended air quality levels. Conscious that this will be a difficult task for many countries and regions struggling with high air pollution levels, WHO has proposed interim targets to facilitate stepwise improvement in air quality and thus gradual, but meaningful, health benefits for the population.
Almost 80% of deaths related to PM₂.₅ could be avoided in the world if the current air pollution levels were reduced to those proposed in the updated guideline, according to a rapid scenario analysis performed by WHO. At the same time, the achievement of interim targets would result in reducing the burden of disease, of which the greatest benefit would be observed in countries with high concentrations of fine particulates (PM₂.₅) and large populations.
Whilst not legally-binding, like all WHO guidelines, AQGs are an evidence-informed tool for policy-makers to guide legislation and policies, in order to reduce levels of air pollutants and decrease the burden of disease that results from exposure to air pollution worldwide. Their development has adhered to a rigorously defined methodology, implemented by a guideline development group. It was based on evidence obtained from six systematic reviews that considered more than 500 papers. The development of these global AQGs was overseen by a steering group led by the WHO European Centre for Environment and Health.
The World Health Organization provides global leadership in public health within the United Nations system. Founded in 1948, WHO works with 194 Member States, across six regions and from more than 150 offices, to promote health, keep the world safe and serve the vulnerable. Our goal for 2019-2023 is to ensure that a billion more people have universal health coverage, to protect a billion more people from health emergencies, and provide a further billion people with better health and wellbeing.
19 September 2021, Beirut, Lebanon – We have just concluded a two-day visit to Beirut, Lebanon to reiterate our commitment to the people of Lebanon and express our solidarity and continued support.
Since the Beirut port blast last year, the country and its people have slipped even further into despair. The current economic crisis has increased poverty across the country, and all sectors including health, are at risk of collapse.
Fuel shortages are causing most hospitals to operate at only 50% capacity. Just today, we were told that two open heart surgeries were cancelled because of limited fuel at the facility where they were planned to take place. Basic and life-saving medicines are in short supply, with restrictions in foreign currency severely limiting importation of medicines and medical goods.
A brain drain is occurring at alarming speed. Almost 40% of skilled medical doctors and almost 30% of registered nurses have already left the country either permanently or temporarily. Mental health needs are greater than ever before, and the ongoing COVID-19 pandemic continues to create additional challenges for both the health sector and communities alike.
The challenges before us are immense and threaten the many significant health gains that Lebanon had made over the last decades. But we can use this crisis as an opportunity to build a better health care system in Lebanon, and work with national authorities, partners, and the international community for positive health sector reform.
We cannot afford to leave behind those most vulnerable and in need. Access to essential and life-saving health services must be preserved at all costs – including for migrants and persons with disabilities.
Throughout our visit, we saw firsthand the spirit of resilience and determination that the Lebanese people are renowned for. Health care workers that have remained in the country are saving lives with the few resources they have at their disposal. The Lebanese people are eager to rebuild their country, and we are with them every step of the way.
At WHO, we have championed the importance of building and maintaining partnerships among the diverse group of players involved in global health — country governments, donors, the private sector, civil society and academics — to overcome barriers to achieving universal health coverage.
We remain committed to continuing our immediate, lifesaving work in Lebanon, while also planning for longer-term strategies for health. And we count on the support of all sectors and all stakeholders to build on the support they have provided so far, so that together, we can take Lebanon from its current crisis to a future where all people can enjoy health as a basic right.
The World Health Organization provides global leadership in public health within the United Nations system. Founded in 1948, WHO works with 194 Member States, across six regions and from more than 150 offices, to promote health, keep the world safe and serve the vulnerable. Our goal for 2019-2023 is to ensure that a billion more people have universal health coverage, to protect a billion more people from health emergencies, and provide a further billion people with better health and wellbeing.
WHO Director-General Tedros Adhanom Ghebreyesus recognizes Mr Brown as a leader who can shape and drive a future of robust, equitable investment in global public health The World Health Organization today announced the appointment of The Rt Hon Gordon Brown, former Prime Minister of the United Kingdom, as WHO Ambassador for Global Health Financing. Mr Brown is widely credited with preventing a second Great Depression through his stewardship of the 2009 London G20 summit. He mobilized world leaders to commit an additional $1.1 trillion to restore credit, growth and jobs to help the world economy through the global financial crisis.
More recently, Mr Brown has tirelessly called on wealthy nations as well as the private sector to ensure the equitable distribution of COVID-19 vaccines, advocating for a concerted global effort -- rooted in science and sound economics – to save lives, end the pandemic and restore livelihoods the world over.
Dr Tedros Adhanom Ghebreyesus, WHO Director-General, hailed Mr Brown as a champion for galvanizing the world’s major economies to protect health and prevent future disease outbreaks.
Dr Tedros said: “I am delighted and honoured that Gordon Brown has agreed to serve as WHO Ambassador for Global Health Financing. In this role, he will elevate and support WHO’s work to raise awareness internationally on the great need for sustained global health financing, particularly from G20 and G7 countries. As a longtime friend of Gordon’s, I know that he will bring his sharp intellect, firm commitment and deep sense of justice to this Ambassadorship.”
Mr Brown said: “I have a tremendous personal regard for Dr Tedros with whom I first worked two decades ago, and I am delighted to be able to help his and WHO’s work raising global finance to ensure everyone has access to health. Our immediate task is to work together to finance the vaccination of the whole world and protect the poorest countries from the terrible effects of COVID-19 and other diseases. ”
Gordon Brown is the United Nations Special Envoy for Global Education and former Prime Minister of the United Kingdom.
He served as Prime Minister of the United Kingdom from 2007 to 2010 and is widely credited with preventing a second Great Depression through his stewardship of the 2009 London G20 summit. He was one of the first leaders during the global crisis to initiate calls for global financial action, while introducing a range of rescue measures in the UK. In April 2009, he hosted the G20 Summit in London where world leaders committed to make an additional $1.1 trillion available to help the world economy through the crisis and restore credit, growth and jobs. They also pledged to strengthen financial supervision and regulation.
Previously, he served as Chancellor of the Exchequer from 1997 to 2007, making him the longest-serving Chancellor in modern history. During ten years at the Treasury, Gordon’s achievements included the Minimum Wage, Sure Start, the Winter Fuel Allowance, the Child Trust Fund, the Child Tax Credit and paid paternity leave. His record on global justice includes his negotiation of debt cancellation for the world’s poorest nations and the tripling of the budget for life-saving aid. His time as Chancellor was also marked by major reform of Britain’s monetary and fiscal policy as well as the sustained investment in health, education and overseas aid.
His role in government continued to shape his views on the importance of education as a fundamental right of every child in the world and the key to unlocking better health, greater social stability, more rights and opportunities for women and a higher standard of living. He is a passionate advocate for global action to ensure education for all. In his role as UN Special Envoy for Global Education, he works closely with key partners to help galvanise support for global education investment and the use of innovative financing to reach the UN’s global goals. He is Chair of the High Level Steering Group for Education Cannot Wait, the fund for education in emergencies; Chair of the Inquiry on Protecting Children in Conflict; and Chair of the International Commission on Financing Global Education Opportunity.
He recently played a key role leading a group of 275 former world leaders, economists and educationalists calling for international action to prevent the global health crisis creating a “COVID generation” - tens of millions of children with no hope of an education.
In addition to his global education work Gordon is an advisor to the Graça Machel Trust, Chair of the Advisory Board at the Catalyst Trust for Universal Education, a Senior Panel Member at the Kofi Annan Foundation initiative on Electoral Integrity, and he is also an Honorary Fellow of the Royal Society of Edinburgh.
Within the United Kingdom, Gordon is also the founder of Our Scottish Future, and the Alliance for Full Employment.
Gordon is the author of several books including Beyond the Crash: Overcoming the First Crisis of Globalisation, My Scotland, Our Britain and My Life, Our Times and most recently, Seven Ways to Change the World (Simon & Schuster, June 2021).
Gordon has a PhD in History from the University of Edinburgh and spent his early career working as a lecturer and in television production. He has been awarded several honorary doctorates, most recently Doctor of the University from The Open University.
He is married to Sarah Brown, the Chair of Theirworld and Executive Chair of the Global Business Coalition for Education, and the couple live in Fife, Scotland with their two sons, John and Fraser.
The World Health Organization provides global leadership in public health within the United Nations system. Founded in 1948, WHO works with 194 Member States, across six regions and from more than 150 offices, to promote health, keep the world safe and serve the vulnerable. Our goal for 2019-2023 is to ensure that a billion more people have universal health coverage, to protect a billion more people from health emergencies, and provide a further billion people with better health and wellbeing.
On 16 September 2021, the Ministry of Health of Guinea declared the end of the Marburg virus disease outbreak in Guéckédou prefecture, Nzérékoré Region. In accordance with WHO recommendations, the declaration was made 42 days after the safe and dignified burial of the only confirmed patient reported in this outbreak. This was the first-ever Marburg virus disease case reported in Guinea.
From 3 August 2021 to the end of outbreak declaration, only one confirmed case was reported. The patient, a man, had onset of symptoms on 25 July. On 1 August he went to a small health facility near his village, with symptoms of fever, headache, fatigue, abdominal pain and gingival hemorrhage. A rapid diagnostic test for malaria returned a negative result, and the patient received ambulatory supportive care with rehydration and symptomatic treatment. Upon returning home, his condition worsened, and he died on 2 August. An alert was subsequently raised by the sub-prefecture public health care facility to the prefectorial department of health in Guéckédou. The investigation team was immediately deployed to the village to conduct an in-depth investigation and collected a post-mortem oral swab sample, which was shipped on the same day to the viral hemorrhagic fever laboratory in Guéckédou city. On 3 August, the sample tested positive for Marburg virus disease by reverse transcriptase-polymerase chain reaction (RT-PCR) and negative for Ebola virus disease. The deceased patient was buried safely and with dignity on 4 August, with the support of the national Red Cross.
On 5 August, the National Reference Laboratory in Conakry provided confirmation by real-time PCR of the positive Marburg result, and on 9 August, the Institut Pasteur Dakar in Senegal provided an additional confirmation that the result was positive for Marburg virus disease and negative for Ebola virus disease.
The Ministry of Health activated the national and district emergency management committees to coordinate the response and engage with the community. Additionally, the Ministry of Health together with WHO, the United States Centers for Disease Control, the Alliance for International Medical Action, the Red Cross, UNICEF, the International Organization for Migration, and other partners, initiated measures to control the outbreak and prevent further spread including the implementation of contact tracing and active case search in health facilities and at the community level.
During the outbreak, a total of one confirmed case who died, (CFR=100%) and 173 contacts were identified, including 14 high risk contacts based on exposure. Among them, 172 were followed for a period of 21 days, of which none developed symptoms. One high-risk contact was lost to follow up. At the different points of entry in Guéckédou prefecture where passengers were screened, no alerts were generated.
Ongoing activities include:
Capturing and sampling of bats in the localities of Temessadou M´Boké, Baladou Pébal and Koundou to better understand the involvement of bats in the ecology of Marburg viruses;
Development of a sero-surveillance protocol in the sub-prefecture of Koundou;
Development and implementation of plans to strengthen Infection Prevention and Control (IPC) programmes at the national and facility level including establishing and mentoring of IPC focal persons, IPC/hygiene committees, ongoing training of health workers and adequate procurement and distribution of supplies such as personal protective equipment (PPE);
Implementation of water, sanitation and hygiene measures with partners including in health facilities and communities;
Supporting training on community-based surveillance in Guéckédou prefecture; and
Risk communication and community mobilization activities in Guéckédou prefecture as a component of a health emergency preparedness and response action plan.
Marburg virus disease (MVD) is an epidemic-prone disease associated with high case fatality ratios (CFR 24-90%). In the early course of the disease, clinical diagnosis of MVD is difficult to distinguish from many other tropical febrile illnesses, because of the similarities in the clinical symptoms. Other viral hemorrhagic fevers need to be excluded, particularly Ebola virus disease (EVD), as well as malaria, typhoid fever, leptospirosis, rickettsial infection and plague. MVD is transmitted by direct contact with the blood, bodily fluids and/or tissues of infected persons or wild animals (e.g., monkeys and fruit bats).
Investigations are ongoing to identify the source of the infection. Guinea has previous experience in managing viral hemorrhagic diseases such as EVD and Lassa fever, but this was the first time that MVD was reported. The country has a fragile health care system due to the overburden of disease outbreaks, COVID-19 pandemic, and the recurrent threat of epidemics such as malaria, yellow fever, measles, Lassa fever, EVD, health care-associated infections, high rates of acute malnutrition, cyclical natural disasters such as floods, and socio-political unrest.
Guinea health authorities responded rapidly to the event, and measures were rapidly implemented to control the outbreak. Cross-border population movement and community mixing between Guinea and neighboring Sierra Leone and Liberia increased the risk of cross-border spread. Sierra Leone and Liberia health authorities activated contingency plans and started public health measures at the points of entry with Guinea.
The affected village is in a remote forest area located at the border with Sierra Leone, about 9 km from a main international border crossing point between the two countries. The proximity of the affected area to an international border, cross-border movement between the affected district and Sierra Leone, and the potential transmission of the virus between bat colonies and humans posed an increased risk for cross-border spread.
These factors suggested a high risk at the national and regional level, and given that Guéckédou prefecture is well connected to Foya in Liberia, and Kailahun in Sierra Leone, this outbreak required an immediate and coordinated response with support from international partners. The risk associated with the event at the global level was assessed as low.
Human-to-human transmission of Marburg virus is primarily associated with direct contact with blood and/or bodily fluids of infected persons, and Marburg virus transmission associated with the provision of health care has been reported when appropriate infection control measures have not been implemented.
Health care workers caring for patients with suspected or confirmed Marburg virus disease should apply standard and transmission-based IPC precautions to avoid any exposure to blood and/or bodily fluids, as well as unprotected contact with the possibly contaminated environment. IPC precautions include:
Early recognition (screening, triage) and isolation of suspected cases;
Appropriate isolation capacity (including infrastructure and human resources);
Health care workers’ access to hand hygiene resources (i.e., soap and water or alcohol-based hand rub);
Appropriate and accessible PPE for health care workers;
Safe infection practices (emphasize on single-use only needles);
Procedures and resources for decontamination and sterilization of medical devices; and
Appropriate management of infectious waste.
IPC assessments of health facilities in affected areas using the IPC Scorecard revealed sub-optimal results highlighting the need for ongoing supportive supervision and mentorship for implementation of IPC in health care settings in addition to implementing IPC minimum requirements to support and strengthen future preparedness for emerging and re-emerging infectious diseases.
Integrated disease surveillance and response activities, including community-based surveillance must continue to be strengthened within all affected health zones.
Raising awareness of the risk factors for Marburg virus disease and the protective measures individuals can take to reduce human exposure to the virus are the key measures to reduce human infections and deaths. Key public health communication messages include:
Reducing the risk of human-to-human transmission in the community arising from direct contact with infected patients, particularly with their bodily fluids;
Avoiding close physical contact with patients who have Marburg virus disease;
Any suspected case ill at home should not be managed at home, but immediately transferred to a health facility for treatment and isolation. During this transfer, health care workers should wear appropriate PPE;
Regular hand washing should be performed after visiting sick relatives in hospital; and
Communities affected by Marburg should make efforts to ensure that the population is well informed, both about the nature of the disease itself to avoid further transmission, community stigmatization, and encourage early presentation to treatment centers and other necessary outbreak containment measures, including safe burial of the dead. People who have died from Marburg should be promptly and safely buried.
To reduce the risk of wildlife-to-human transmissions, such as through contact with fruit bats, monkeys, and apes:
Handle wildlife with gloves and other appropriate protective clothing;
Cook animal products such as blood and meat thoroughly before consumption and avoid consumption of raw meat; and
During work, research activities or tourist visits in mines or caves inhabited by fruit bat colonies, people should wear gloves and other appropriate protective clothing including masks.
The World Health Organization provides global leadership in public health within the United Nations system. Founded in 1948, WHO works with 194 Member States, across six regions and from more than 150 offices, to promote health, keep the world safe and serve the vulnerable. Our goal for 2019-2023 is to ensure that a billion more people have universal health coverage, to protect a billion more people from health emergencies, and provide a further billion people with better health and wellbeing.
Fourth Meeting of the Multilateral Leaders Task Force on Scaling COVID-19 Tools
The heads of the International Monetary Fund, World Bank Group, World Health Organization and World Trade Organization met with the CEOs of leading vaccine manufacturing companies to discuss strategies to improve the access to COVID-19 vaccines, especially in low- and lower middle-income countries and in Africa. The Task Force expressed concerns that without urgent steps the world is unlikely to achieve the end-2021 target of vaccinating at least 40% of the population in all countries—a critical milestone to end the pandemic and for global economic recovery.
The Task Force members noted that, despite adequate total global vaccine production in the aggregate, the doses are not reaching low- and lower middle-income countries in sufficient amounts, resulting in a crisis of vaccine inequity. The Task Force encouraged countries that have contracted high amounts of vaccine doses, and vaccine manufacturers, to come together in good faith to urgently accelerate COVID-19 vaccine supplies to COVAX and AVAT, two multilateral mechanisms that are crucial for equitable distribution of vaccines.
Task Force members welcomed the willingness of the CEOs to work collectively with them to end vaccine inequity and their readiness to form a technical working group with the Task Force to exchange and coordinate information on vaccine production and deliveries.
The Task Force stressed that if the 40% coverage threshold is to be reached in all countries by the end of 2021, the following actions need to be taken immediately by governments and vaccine manufacturers:
Release doses to low- and lower middle-income countries: Task Force members take note that countries with high vaccination rates have collectively pre-purchased over two billion doses in excess of what is required to fully vaccinate their populations. The Task Force calls again on those countries to urgently: i) swap their near-term delivery schedules with COVAX and AVAT, ii) fulfill their dose donation pledges with unearmarked upfront deliveries to COVAX, and iii) release vaccine companies from options and contracts so those doses can be delivered to people in low- and lower middle-income countries. In addition, vaccine manufacturers should prioritize and fulfill their contracts to COVAX and AVAT.
Transparency on supply of vaccines: To ensure that doses reach countries that need them the most, particularly low- and lower middle-income countries, the Task Force calls on vaccine manufacturers to share details on month-by-month delivery schedules for all vaccine shipments, especially for COVAX and AVAT. In its remarks, WHO emphasized its call for a moratorium on booster doses until the end of 2021, with the exception of the immune-compromised, to help optimize supply to low-income countries.
Eliminate export restrictions, prohibitions: The Task Force calls on all countries to urgently address export restrictions, high tariffs and customs bottlenecks on COVID-19 vaccines and the raw materials and supplies required for the production and timely distribution of vaccines.
Regulatory streamlining and harmonization: The Task Force calls on all regulatory authorities around the world to create regulatory consistency and standardization on the approval of vaccines, and to support the acceptance of the WHO Emergency Use Listing procedure. In parallel, efforts should be made to boost production of vaccines, diagnostics and treatments globally and expedite equitable delivery of such lifesaving tools to developing countries.
The World Health Organization provides global leadership in public health within the United Nations system. Founded in 1948, WHO works with 194 Member States, across six regions and from more than 150 offices, to promote health, keep the world safe and serve the vulnerable. Our goal for 2019-2023 is to ensure that a billion more people have universal health coverage, to protect a billion more people from health emergencies, and provide a further billion people with better health and wellbeing.
An aircraft carrying around 23 metric tonnes of life-saving medicines and supplies from WHO landed in Kabul today at 13:30 local time.
The shipment, which is among the first humanitarian aid to arrive at Kabul airport since operations were disrupted on 15 August, was flown by a Qatar Airways flight donated by the Government of the State of Qatar.
“As health needs increase in Afghanistan, we must move quickly to address the shortages in medical supplies to keep life-saving health services running. I thank the Government of the State of Qatar for its generous and timely support, which has allowed WHO to replenish depleted stocks and meet the needs of the most vulnerable Afghans,” said Dr Tedros Adhanom Ghebreyesus, Director-General of the World Health Organization.
A second flight donated by the State of Qatar is expected to arrive later this week, carrying more WHO medical supplies.
Together, the 2 shipments which contain essential medicines such as insulin, medical consumables, trauma and surgery kits, and COVID-19 testing kits, will address the urgent health needs of 1.45 million people and provide for 5400 major and minor surgeries. They will be distributed to 280 health facilities and 31 public COVID-19 laboratories across Afghanistan.
The supplies have been shipped from WHO suppliers’ facilities in Europe to Qatar and onward to Kabul, Afghanistan, in collaboration with the operations and logistic teams of Qatar Airways and the Government of the State of Qatar.
WHO is exploring options to expedite further shipments of health supplies to Afghanistan.
The establishment of a reliable humanitarian airbridge continues to be a pressing need to ensure timely movement of humanitarian aid and personnel to respond to the evolving situation.
WHO is committed to staying and delivering. The 2 flights from Qatar will mean that WHO will have airlifted 131 metric tonnes of supplies since 30 August, which are enough to cover the urgent health needs of 2.43 million people and provide for around 19 000 major and minor surgeries.
The World Health Organization provides global leadership in public health within the United Nations system. Founded in 1948, WHO works with 194 Member States, across six regions and from more than 150 offices, to promote health, keep the world safe and serve the vulnerable. Our goal for 2019-2023 is to ensure that a billion more people have universal health coverage, to protect a billion more people from health emergencies, and provide a further billion people with better health and wellbeing.
14 September 2021, Geneva – WHO Director-General Dr Tedros Adhanom Ghebreyesus and a group of global health leaders today issued an urgent call for vaccine equity globally and in Africa in particular. The leaders stressed that the worst pandemic in the last hundred years will not end unless and until, there is genuine global cooperation on vaccine supply and access. They also reiterated the WHO’s global vaccination target for 70% of the population of all countries to be vaccinated by mid-2022.
Dr Tedros was joined by Dr Seth Berkley, CEO Gavi, Strive Masiyima, AU Special Envoy for COVID- 19, Dr John Nkengasong, Africa CDC Director, Professor Benedict Oramah, President and Chairman of the Board of Directors, Afreximbank, Dr Vera Songwe, UN Under- Secretary- General and Executive Secretary of the Economic Commission For Africa and Dr Matshidiso Moeti, WHO Regional Director for Africa.
The press conference followed two days of meetings among the leaders, with Richard Hatchett, Chief Executive Officer of CEPI joining the meetings as well.
Selected quotes:
Dr Tedros Adhanom Ghebreyesus: Director-General, WHO
“More than 5.7 billion doses have been administered globally, but only 2% of those have been administered in Africa.”
“This doesn’t only hurt the people of Africa, it hurts all of us. The longer vaccine inequity persists, the more the virus will keep circulating and changing, the longer the social and economic disruption will continue, and the higher the chances that more variants will emerge that render vaccines less effective.”
Strive Masiyima, AU Special Envoy for COVID-19
"Vaccine sharing is good but we shouldn't have to be relying on vaccine sharing. Particularly when we can come to the table, put structures in place and say, we also want to buy."
"American taxpayers, European taxpayers, they financed some of this intellectual property and it should be for the common good. So, it is not wrong that we say there should be waivers, it was for the common good. So, we ask for this IP to be made available."
"It was a great miracle to have these vaccines, now let this miracle be available to all mankind."
Dr John Nkengasong, Africa CDC Director
“We will not be able to achieve 60% of our population fully immunised if we do not fully explore and deploy the power of partnership, the power of cooperation, and the power of solidarity” … “We all have acknowledged now that vaccines are the only solution for us to get out of this pandemic collectively. That has to be done quickly.”
Dr Vera Songwe, UN Under- Secretary- General and Executive Secretary of the Economic Commission For Africa
“For every one month of lockdowns in the continent cost us $29 billion of production that was lost. For [the African continent], when we say that COVID-19 is an economic issue and we need to respond to it, to be able to recover and reset our economies, it is real. And for that we need financing and we need to see how we can bring together global financial structures to ensure that we can actually respond to this crisis”.
“We know that scarcity means increased cost, and we cannot afford today as a continent that kind of scarcity.”
Professor Benedict Oramah, President and Chairman of the Board of Directors, Afreximbank
“Africa did not want to once again be at the bottom of queue in regard to vaccines because it was well known to everybody that economy recovery meant bringing the virus under control.”
“It is important that we do this for the simple reason that countries want us to make sure that we do not fail, and make it difficult for us to recover quickly.”
Dr Seth Berkley, CEO Gavi
“Today’s meeting is important, as it symbolizes the spirit of partnership between COVAX, the African Union and AVATT: Africa needs more doses and together we will get them.”
“We're poised to embark on the busiest period of what is the largest and most complex vaccine rollout in history. We've demonstrated that COVAX can work at scale, but it's really time for the world to get behind it.”
Dr Matshidiso Moeti, WHO Regional Director For Africa
“The question is sometimes asked do African countries have the capacity to absorb the vaccines? The simple answer is yes. The continuous challenge is that global supplies are not being shared in ways that will get the world out of this pandemic.”
“Hundreds of WHO staff are on the ground, ready to support countries to expand vaccination sites and to manage the complexities of small deliveries of a variety of vaccines“.
“What’s more, African countries have done this before – successfully implementing massive vaccination campaigns against polio, yellow fever and cholera.”
Notes for Editors
WHO’s targets are to vaccinate at least 10% of the population of every country by September, at least 40% by the end of the year, and 70% globally by the middle of next year. These are the critical milestones we must reach together to end the pandemic.
Almost 90% of high-income countries have now reached the 10% target, and more than 70% have reached the 40% target. Not a single low-income country has reached either target.
Globally, 5.5 billion vaccine doses have been administered, but 80% have been administered in high- and upper-middle income countries.
High-income countries have now administered almost 100 doses for every 100 people. Meanwhile, low-income countries have only been able to administer 1.5 doses for every 100 people, due to lack of supply.
The world should spare no effort to increase vaccine supply for lower-income countries: this can be done by removing all the barriers to scaling up manufacturing including waiving IP, freeing up supply chains and technology transfer. As part of these efforts, in June, WHO and COVAX partners announced the first COVID mRNA vaccine technology transfer hub, to be set up in South Africa.
High-income countries have promised to donate more than 1 billion doses, but less than 15% of those doses have materialised and manufacturers have promised to prioritize COVAX and low-income countries.
The supply through COVAX and other sources will increase substantially in the coming months of this year. Countries need to prepare for this ramp up of available doses, for example with microplanning, expanded cold chain equipment, logistics, funding, and trained staff in place.
COVAX has shipped more than 236.6 million doses to 139 participants as of 6th September 2021. Some 41 participants started their first campaigns thanks to COVAX.
Safe and effective vaccines alone cannot solve the pandemic: Robust surveillance supported by rapid diagnostics, early clinical care and life- saving therapeutics, provided by well-trained health workers who are able to work in safe conditions. Public health and social measures are also vital to end the pandemic and accelerate global recovery.
The World Health Organization provides global leadership in public health within the United Nations system. Founded in 1948, WHO works with 194 Member States, across six regions and from more than 150 offices, to promote health, keep the world safe and serve the vulnerable. Our goal for 2019-2023 is to ensure that a billion more people have universal health coverage, to protect a billion more people from health emergencies, and provide a further billion people with better health and wellbeing.
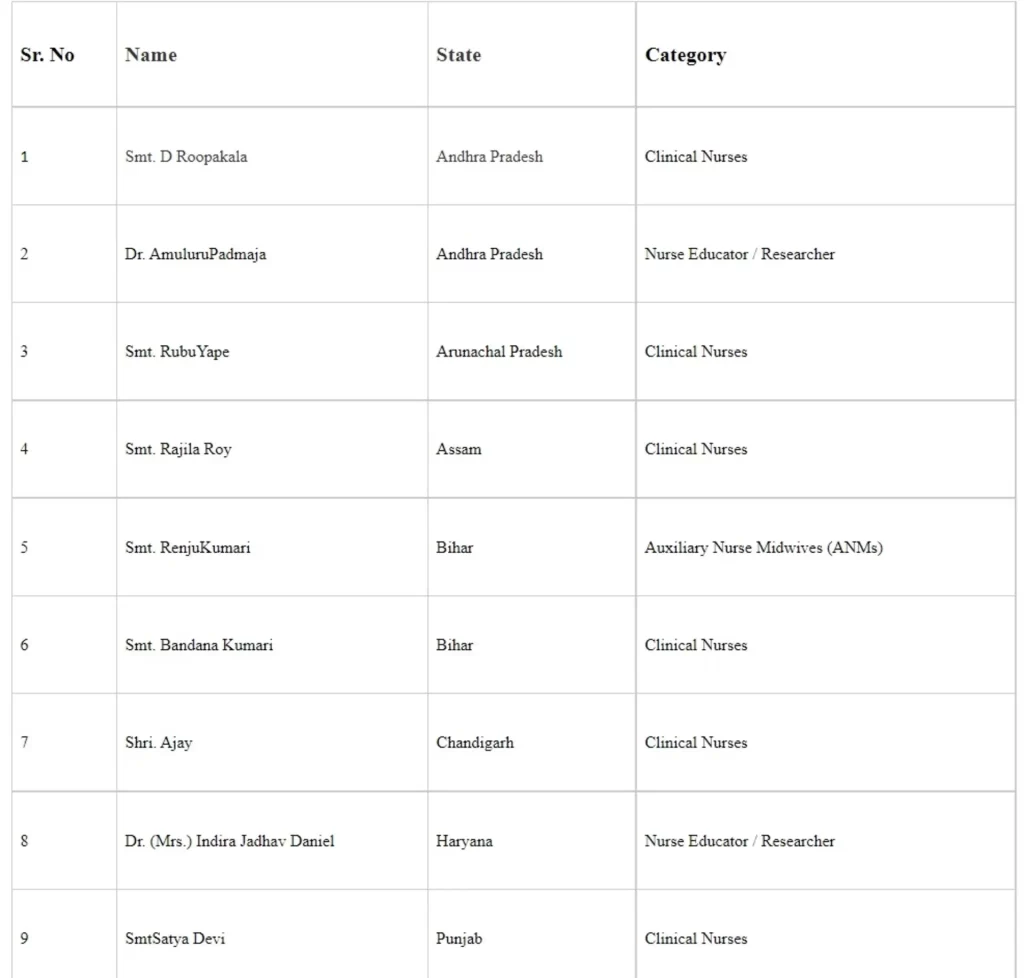
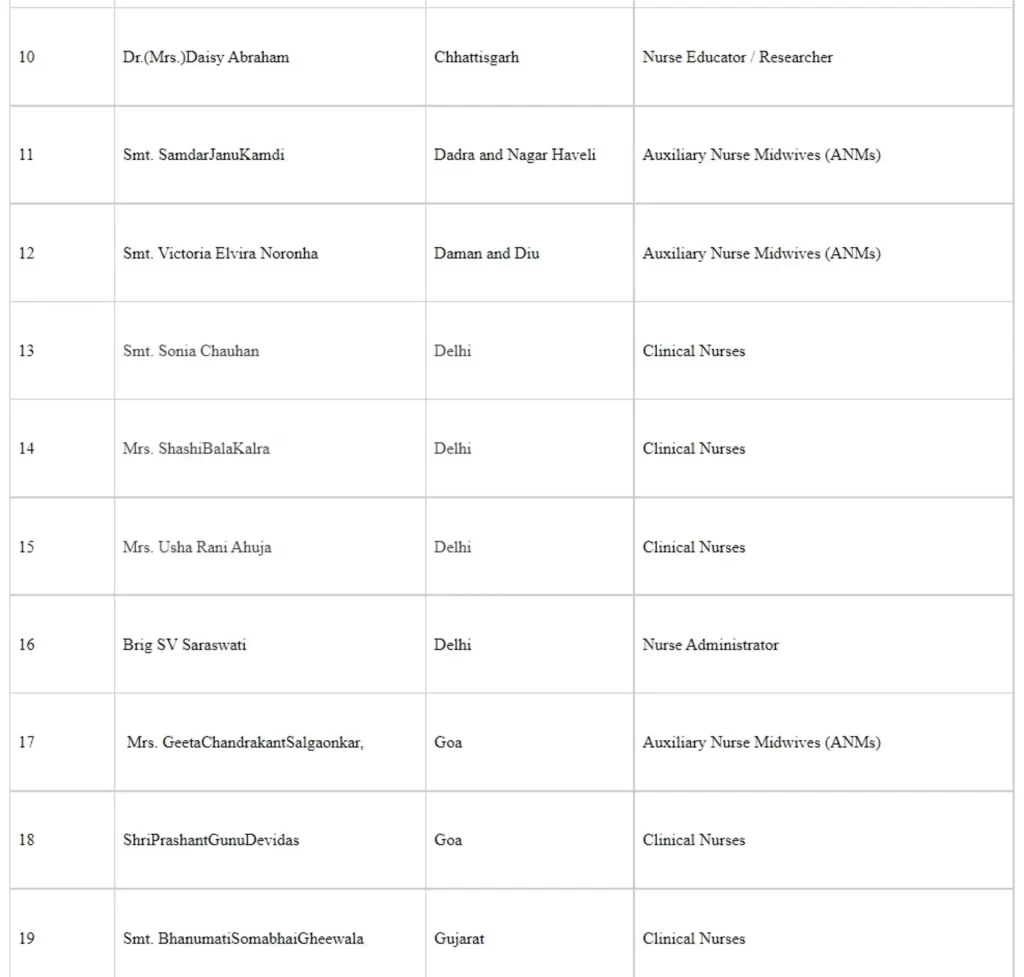
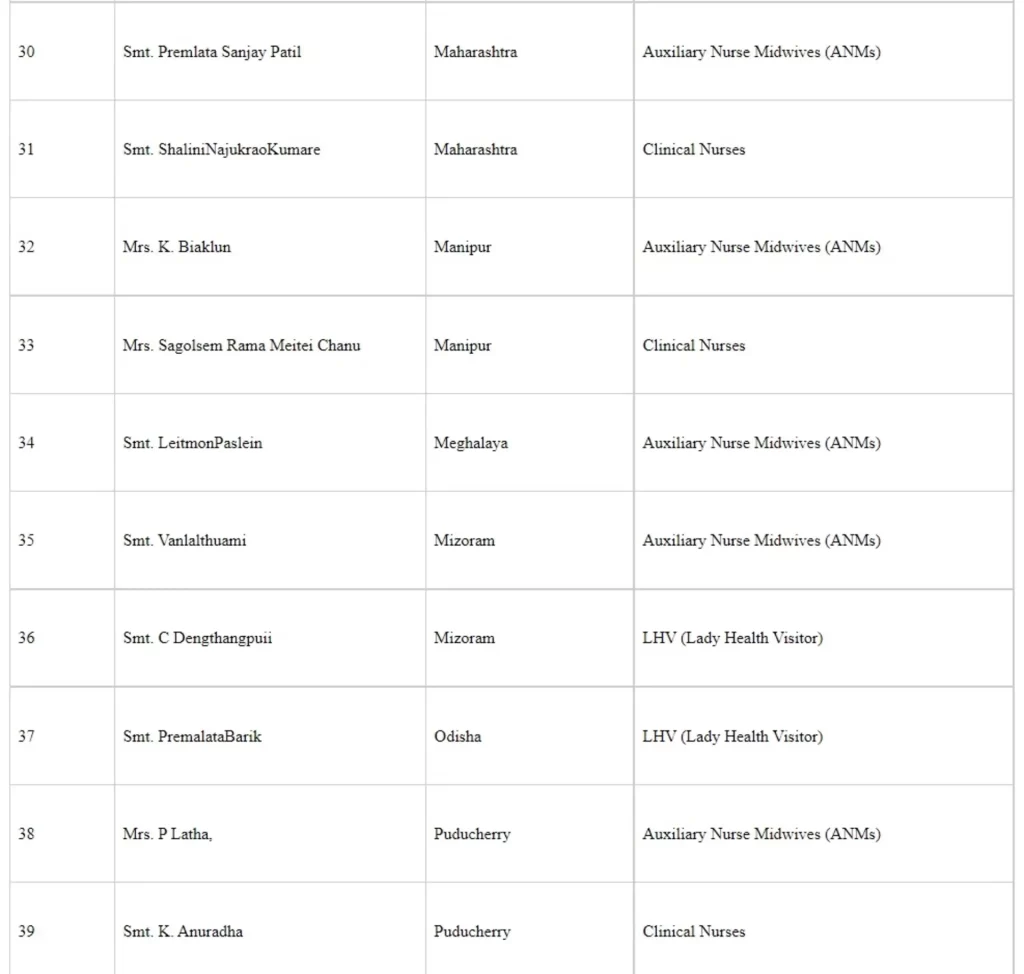
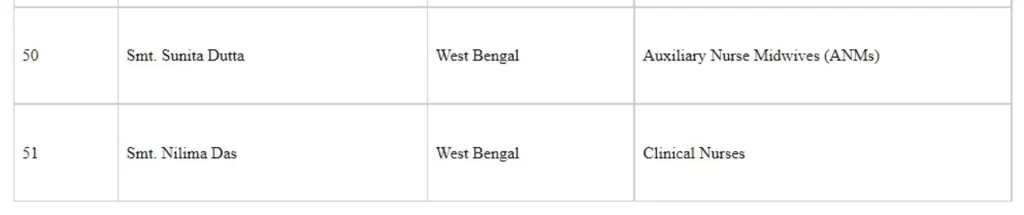
The President of India, Shri Ram Nath Kovind conferred the National Florence Nightingale Awards 2020 to 51 awardees at a virtual ceremony, in the presence of Shri Mansukh Mandaviya, Union Minister of Health & Family Welfare and Dr. Bharati Pravin Pawar, Union Minister of State for Health & Family Welfare.

Congratulating all the health care workers and nurses, The President noted ancient Indian traditions of service and helping the needy which are reflected in the service of our nurses. The President exemplified the selfless contribution of nurses in the gallant fight against COVID-19 as well as their hard work in accelerating the national COVID Vaccination Programme. He added that more than one crore vaccine doses per day has become possible by the exemplary devotion of our nurses. “Your hard-work is a ray of hope and guide people towards light from darkness,” he said. Paying tribute to those who lost their lives, he observed, “Nation will be indebted to your service.”
The President underlined various initiatives taken by the Government such as Midwifery service and insurance scheme under Pradhan Mantri Gareeb Kalyaan Yojana for the health workers. As a vital element in health care delivery, the President acknowledged nurses as the first link between public and health care system.
Echoing the same sentiments, Union Health Minister Shri Mansukh Mandaviya highlighted how 2020 brought the huge challenge of corona pandemic to the whole world. He stated that Prime Minister Shri Narendra Modi has on several occasions appreciated the contribution of nurses during the COVID pandemic in his address to the nation. He recounted his recent visit to Italy to attend the G-20 health ministers meeting where he highlighted the selfless dedication of the nurses working round the clock during the Corona epidemic. “The human spirit, loyalty and selflessness with which you are serving people are commendable,” he stated. The nursing professionals form one of the most important and crucial pillars of healthcare delivery system, he added. He offered condolences to those who have lost their lives while serving those who were suffering from COVID.
Dr. Bharati Pravin Pawar while giving the vote of thanks expressed gratitude to all the nurses and the COVID warriors who have worked tirelessly during the most trying of times to save lives.
Shri Rajesh Bhushan, Union Health Secretary and other senior officials of the Ministry were also present at the event.
Florence Nightingale awards were instituted in the year 1973 by the Government as a mark of recognition for the meritorious services rendered by nurses to the society.
The event was webcast at https://webcast.gov.in/events/MTQzMQ--/session/MzM2Ng--
The address of the Union Health Minister can be viewed at https://youtu.be/f0u1KTtf8Kc
The achievements of the awardees can be viewed at - https://www.youtube.com/watch?v=4zBdZr170eQ
The following healthcare workers were commended for their work and were awarded the National Florence Nightingale awards 2020 (Seriatum wise)


Kinshasa – The Democratic Republic of the Congo has declared an outbreak of meningitis in the north-eastern Tshopo Province where 261 suspected cases and 129 deaths—a high case fatality ratio of 50%—have been reported.
Confirmatory tests carried out by the Institut Pasteur in Paris detected Neisseria meningitidis – one of the most frequent types of bacterial meningitis with the potential to cause large epidemics.
The health authorities have deployed an initial emergency team, and with the support of the World Health Organization (WHO), efforts are underway to quickly ramp up the response. A crisis response committee has been set up in Banalia, the community affected by the outbreak, as well as in Kisangani, the capital of Tshopo, to accelerate the outbreak control efforts. WHO has provided medical supplies in Banalia and plans to deploy more experts and resources.
“Meningitis is a serious infection and a major public health challenge. We are moving fast, delivering medicines and deploying experts to support the government’s efforts to bring the outbreak under control in the shortest possible time,” said Dr Matshidiso Moeti, WHO Regional Director for Africa.
More than 100 patients are already receiving treatment at home and in health centres in Banalia. Meningitis is transmitted among people through droplets of respiratory or throat secretions from infected people. Close and prolonged contact or living in close quarters with an infected person facilitates the spread of the disease. Although people of all ages can catch the disease, it mainly affects babies, children and young people.
“We are scaling up control measures within the community and rapidly investigating suspected cases in surrounding localities to treat patients and curb potentially widespread infections,” said Dr Amédée Prosper Djiguimdé, WHO Representative in the Democratic Republic of the Congo.
More than 1.6 million people aged between 1 and 29 years were vaccinated in a massive campaign in 2016 in Tshopo, which lies in the African meningitis belt that runs across the continent from Senegal to Ethiopia and comprises 26 countries. The African meningitis belt is the most vulnerable globally to recurrent outbreaks.
Meningitis outbreaks have occurred in several provinces of the Democratic Republic of Congo in the past. In 2009, an outbreak in Kisangani infected 214 people and caused 15 deaths—a case fatality ratio of 8%.
Meningitis is potentially fatal and is a medical emergency. Admission for treatment is necessary and appropriate antibiotic treatment must be started as soon as possible. Over the years, major improvements have been made on vaccines, which are specific to the type of meningitis.
In November 2020, the World Health Assembly—the global health policy-setting body—approved a roadmap for a meningitis-free world by 2030, with three key objectives: elimination of bacterial meningitis, reduction of vaccine-preventable bacterial meningitis by 50% and deaths by 70%, as well as reduction of disability and improvement of quality of life after meningitis.
The World Health Organization provides global leadership in public health within the United Nations system. Founded in 1948, WHO works with 194 Member States, across six regions and from more than 150 offices, to promote health, keep the world safe and serve the vulnerable. Our goal for 2019-2023 is to ensure that a billion more people have universal health coverage, to protect a billion more people from health emergencies, and provide a further billion people with better health and wellbeing.